Thyroid Complications
Thyroid dysfunction is a frequent comorbid condition with menopause. By understanding its fundamental relationship with estrogen, women can be better adept for midlife symptom recognition.
Endocrine Function
The thyroid is a gland located in the neck responsible for monitering many vital bodily functions such as temperature, metabolism, and growth. To accomplish this, it produces hormones named free thyroxine (T4) and free triiodothyronine (T3) (Chiasera, 2013).
If the blood stream has a proper saturation of T3 and T4 hormones, the body is deemed at homeostasis, and vice versa.
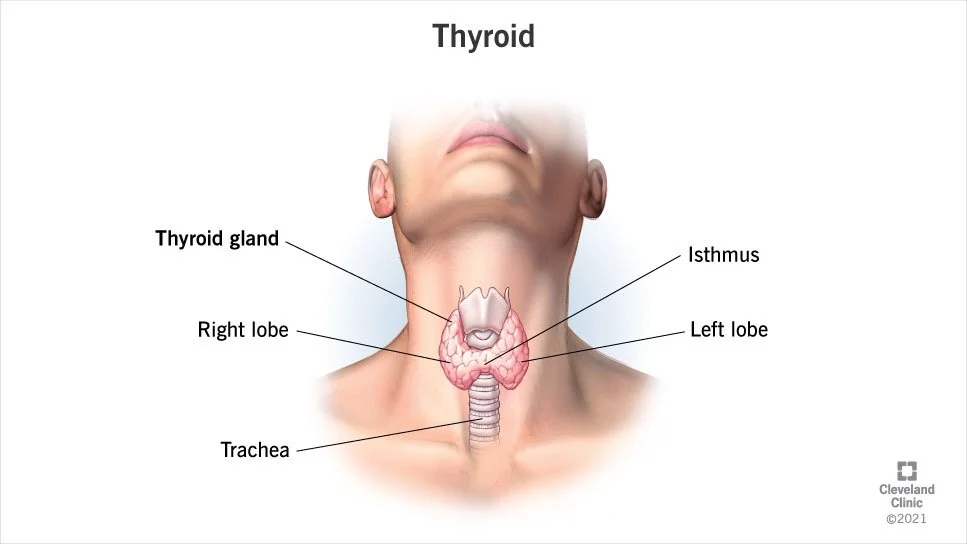
(Cleveland Clinic: Thyroid, 2022)
Signaling Networks
Thyroid hormone production is one factor of the overarching hypothalamus-pituitary-thyroid (HPT) axis. This axis refers to the signaling of the hypothalamus, a small structure beneath the brain responsible for assessing the body’s current thyroid saturation. Depending on this concentration, the hypothalamus releases thyrotropin-releasing hormone (TRH) to the pituitary.
The pituitary gland connects to the hypothalamus at the base of the brain. It physically manifests the hypothalamus’s response to thyroid concentration by proportionally secreting thyroid-stimulating hormone (TSH). This TSH arrives at the thyroid gland to encourage free T3 and T4 production, which then gets interpreted back by the hypothalamus. This cyclical pattern creates the HPT axis (Chiasera, 2013).
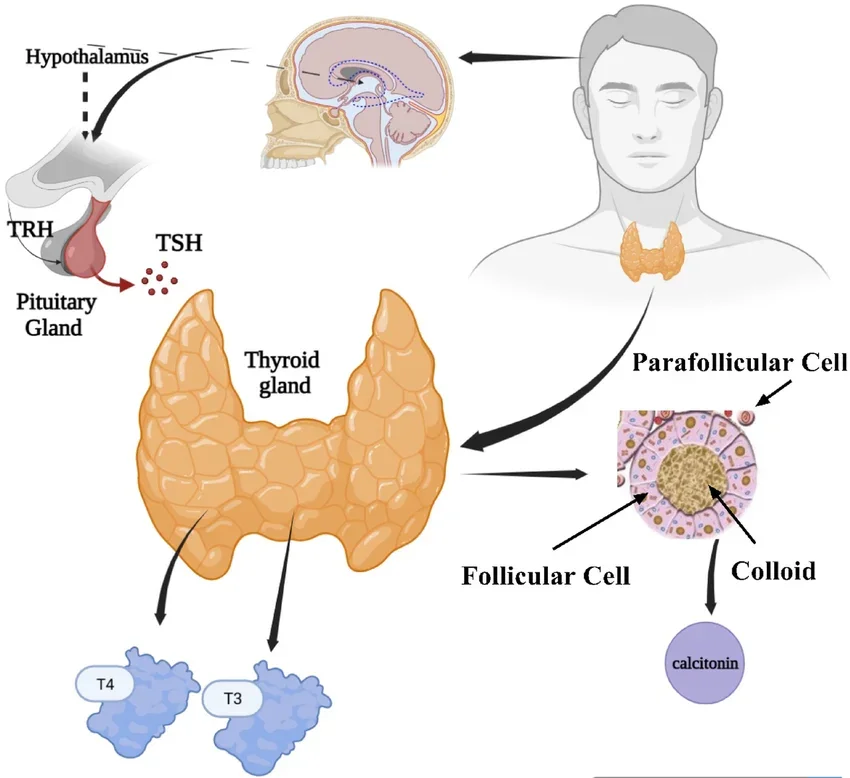
(Adam & Abbas, 2025)
While the HPT axis manages hormone secretion, free thyroid hormones must be processed before entering the bloodstream. This is accomplished in the liver. Given a high concentration of T4 and low concentration of T3 from the thyroid directly, the liver must convert a fraction of the inactive T4 to active T3. Thus, to concentrate the blood in a proper ratio with hormone secretion, T3 and T4 get packaged by thyroxine-binding globulin (TBG).
TBG levels are directly proportional to thyroid concentration: a higher number of TBG proteins creates more binding sites, lowering circulatory T3/T4 concentration and signaling for the hypothalamus to produce TRH. Likewise, a lower number of TBG proteins creates less binding sites, indicating a higher circulatory concentration and signaling for less TRH (Chiasera, 2013).
Thyroid Dysfunction
Like any organ, the thyroid loses its functional abilities with time. Thyroid dysfunction is most commonly caused by autoimmune impairment, inhibiting or inflating T3 and T4 production.
Hypothyroidism
Hypothyroidism occurs when the thyroid underproduces T3 and T4 hormones despite the pituitary’s increased TSH signal. This endocrine behavior is often attributed to Hashimoto’s thyroiditis, a phenomenon in which antibodies attach to and deteriorate the thyroid (Roofs, 2012). Thyroid hormones are elemental to homeostasis, meaning their scarcity reduces functional abilities throughout the body. Common symptoms include but are not limited to:
Muscle weakness
Thinning hair
Slowed heart rate (bradycardia)
Depression
Weight gain
Irregular menstrual cycles (female)
Cold sensitivity/intolerance
Tiredness
Poor memory
(Mayo Clinic: Hypothyroidism, 2022)
Hypothyroidism is especially prevalent in older women; a 2018 study conducted at the North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences observed that hypothyroidism presence increased with age from 23.82% to 62.5% across women 40-70 years old (Das & Panda, 2018).
Hyperthyroidism
Menopause-Thyroid Overlap
Inversely, hyperthyroidism describes an overactive thyroid that abnormally increases the blood’s hormone concentration despite the pituitary’s decreased TSH signal. This condition is often a biproduct of Grave’s disease, an autoimmune attack in which antibodies attach to and overstimulate the thyroid (Roofs, 2012). When the blood has a surplus of active thyroid hormones, the body utilizes this excess to speed up regular processes. As a result, common symptoms include but are not limited to:
Muscle weakness
Increased hunger
Tremor/trembling
Rapid heart rate (tachycardia)
Heart palpitations
Irregular menstrual cycles (female)
Sweating
Weight loss
Heat sensitivity/intolerance
(Mayo Clinic: Hyperthyroidism, 2022)
Hypothyroidism’s prevalence in older women complicates midlife symptom interpretation, primarily because an abnormal thyroid manifests similarly or identically to that of menopause.
Thyroid Dysfunction
Symptom ambiguity can originate from abnormal thyroid behaviors that imitate menopause. A 2023 retrospective study noted that symptoms of menopause, such as hot flashes, increased sweating, sleep disorders, and increased nervousness are commonly associated with thyroid disease (Frank-Raue & Raue, 2023). Specifically, a study analyzing female tertiary patients’ menstrual irregularities with respect to comorbid hypothyroidism found that 55% of women with elevated TSH levels had oligomenorrhea, a state of infrequent menstrual periods (Himabindu et al., 2024). Conditional similarities to this degree make interpretation difficult and at times misleading.
Estrogen Depletion
In some cases, menopause-thyroid overlap does not include the thyroid at all. Beyond symptom overlap, estrogen depletion can explicitly hinder HPT-specific processes. For instance:
Thyrotropin-Releasing Hormone (TRH) → Pituitary TRH receptors face lower expression levels, decreasing TRH sensitivity.
Thyroid-Stimulating Hormone (TSH) → Lower TRH reception reduces TSH secretion.
Thyroid-Binding Globulin (TBG) →TBG loses abundance, increasing circulatory saturation, temporarily signaling for decreased TRH.
(Xie et al., 2025)
Thus, while menopause cannot cause thyroid dysfunction, it provides the means for its network’s temporary infiltration. In doing so, the female body experiences a plethora of symptoms synonymous to menopause and hypothyroidism alike.
The question for older women remains: Are my symptoms representative of estrogen depletion or potential thyroid dysfunction?
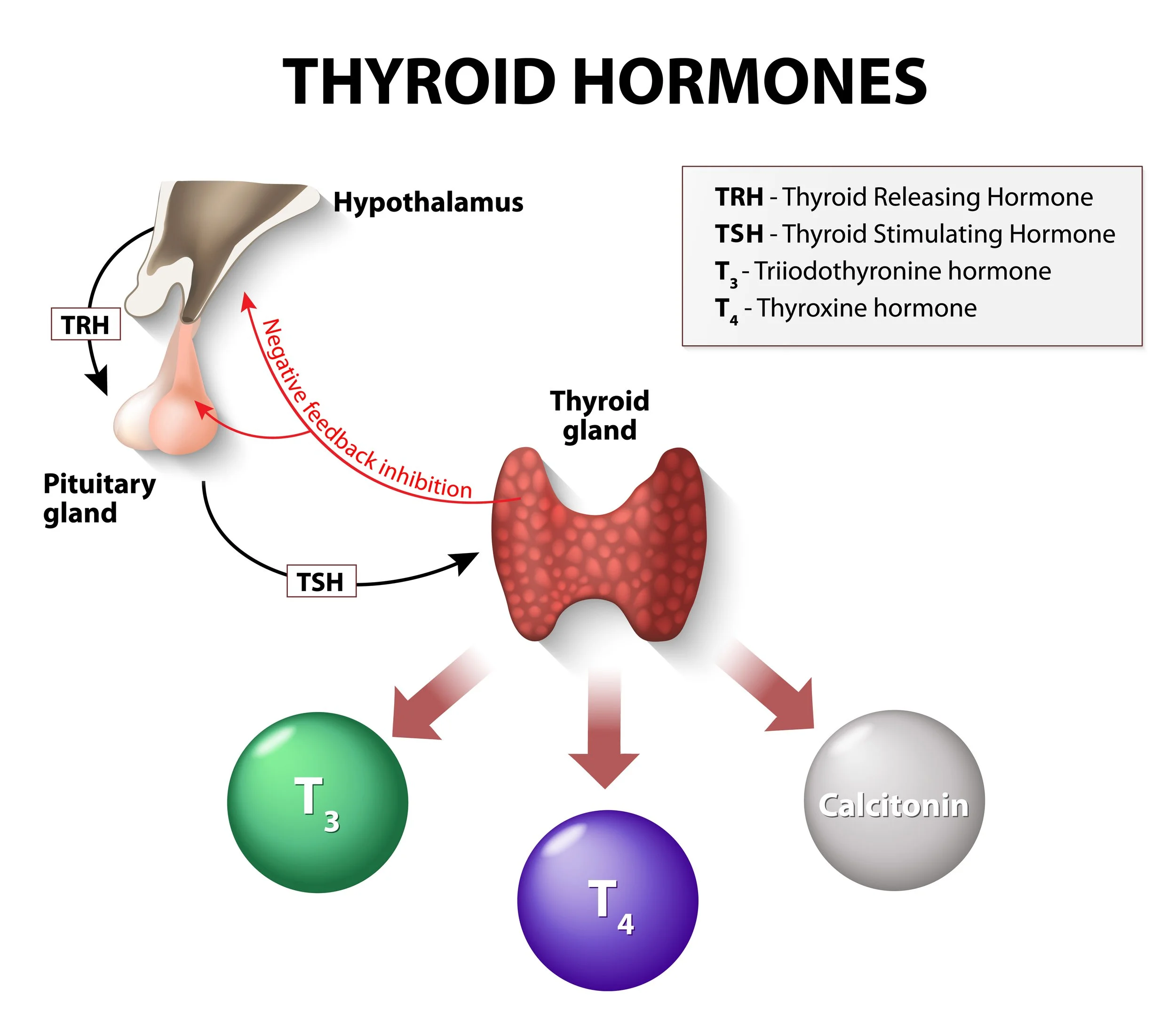
(How thyroid hormones interact)